

Best wishes to you for a happy, healthy and successful 2019. While thinking about the first post for the new year, I decided I would publish this article from
Here is the full article, references and credits, I do not have any commercial relationship with HVMN, I am publishing the article because I believe it dispels some of the perceived evils of fat consumption and promotes a healthy diet.
Leave a comment with your thoughts on the keto diet.
Disclaimer: I may earn a commission should you order other products or services advertised on this blog.

Keto Diet Fundamentals
Originally published on HVMN by Dr. Brianna Stubbs and Nate Martins.
You’ve heard of the keto diet. Everyone from Lebron James to the Kardashians has used the low-carbohydrate, high-fat diet for reasons like performance and weight loss.
The goal of the keto diet is to get the body producing ketones– a fundamentally different energy source than the carbohydrates and fats your cells typically use for energy. It can take several days of ketogenic eating before the body starts to produce ketones. And the time it takes to get into ketosis varies between individuals.
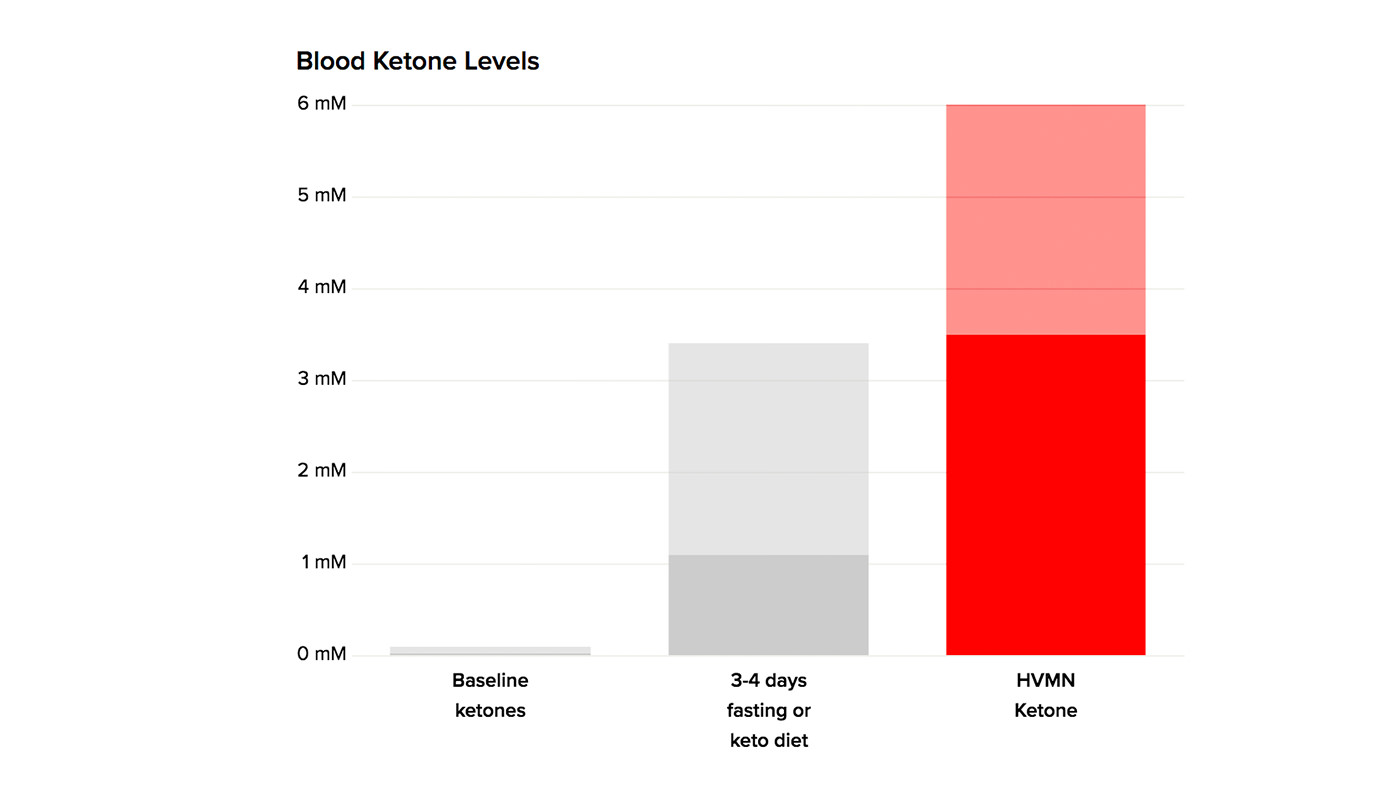
“Keto” comes from the word “ketogenic.” This is a nuanced term meaning that the body is producing ketones from fat.1 When blood ketone levels exceed 0.5mM, the body has achieved “ketosis.” So ketosis can be achieved either through diet or fasting (meaning the body is producing its own ketones to be ketogenic), or also by consuming products that raise blood ketone levels (like HVMN Ketone or ketone salts or MCT oils).
Limiting carb intake and protein intake encourages the body to burn fat–and thus produce ketones. Importantly, restricting proteins as well as carbohydrates limits the amount of substrate available for gluconeogenesis. This is the process of making glucose from non-glucose molecules such as lactate, glycerol, or protein.
Because the ketogenic diet is low-carbohydrate, it often gets confused with other low-carb diets out there. Just because a diet is low carb doesn’t mean it’s keto. It’s subtle differences in the macronutrients provided in the diet determine if the diet is ‘ketogenic.’
A macronutrient is something humans consume in large quantities to provide the bulk of energy to the body. The primary macronutrients are carbohydrates, fats, and proteins. For a diet to be ketogenic, it must be high in fat, low-moderate in protein, and very low in carbohydrates.

Here are some helpful definitions of diets with an element of reduced carbohydrate intake:
Ketogenic Diet
- The aim is to trigger the production of ketones in the body
- High fat, low/moderate protein, and low carbohydrate
Low-Calorie Ketogenic Diet
- The aim is to severely restrict calories to a level below the basic metabolic needs (i.e., <800 kCal)
- Even if this diet is relatively high in carbohydrates, the calorie deficit created can still lead to a state of ketosis
- Not sustainable long-term
Low-Carbohydrate Diet
- Defined in medical literature as a diet with < 30% energy from carbohydrates2
- May not lead to ketosis as the carbohydrate and protein intake could be too high
Atkins Diet
- This diet has several phases
- Initially, the aim is to restrict the carbohydrate intake to less than 20g per day. This degree of restriction is likely to lead to ketosis, although this is not an explicit aim
- Subsequently, the diet reintroduces carbohydrates to a level “the body can tolerate”3
- Less restriction on protein compared to a ‘true ketogenic diet–high fat, moderate protein, low carbohydrate.
Paleo Diet
- The aim is to limit the diet to foods that would have been available to Paleolithic man4
- Wide variability in interpretations
- Foods allowed include vegetables, fruits, nuts, roots, and meat
- Foods excluded include dairy, grains, sugar, legumes, processed oils, alcohol, and coffee
- No structured macronutrient target; however, following a Paleo diet results in higher protein and fat consumption than an average diet
Now you have a grasp of what makes the ketogenic diet unique–but where’d it start?
The History of the Ketogenic Diet
Fasting and Early Pioneers of the Ketogenic Diet
The concept of fasting (taking in zero calories) predates the ketogenic diet as we now understand it. Many of the benefits of fasting are likely due to the presence of ketones in the body.
Since the earliest days of man, fasting has been used as a tool to physically and spiritually cleansing.
The Bible describes fasting as a treatment for convulsions. The ancient Greek philosopher Hippocrates said, “To eat when you are sick is to fuel your sickness.”
Early advocates of fasting were obviously unaware of ketosis as a crucial factor in the anticonvulsant effect of fasting. In the early 1900s, physicians at the Mayo Clinic observed a link between a low-carb diet and fasting. They discovered that severely restricting dietary carbohydrates and increasing fat intake could decrease seizures in the same way as fasting.5 It was not until the mid-1900s, when scientists could measure ketones, that we understood fasting led to the presence of ketones in the body.
Epilepsy was not the only disease historically treated with a low-carbohydrate, high-fat diet. Low-carbohydrate diets were also advocated for patients with diabetes and obesity. Before the discovery of insulin in 1921, diabetes was managed through carbohydrate restriction. William Banting, an obese British mortician, popularized the weight loss benefits of a diet “stripped of starchy foods” in a pamphlet called “Letter on Corpulence, Addressed to the Public.”
The Dark Ages for the Ketogenic Diet
To many, a low-carbohydrate and high-fat diet is a counter-intuitive approach to support health. There is a widespread fear dietary fat is linked to obesity, high blood pressure, high cholesterol levels and other associated health complications.
In 1953 Ancel Keys, an American biochemist published an epidemiological study that introduced the “diet-heart” hypothesis. The study claimed dietary fat was a key risk factor in developing heart disease. The “diet-heart” hypothesis proposed blood LDL and cholesterol derived from dietary fat accelerates the development of atherosclerotic plaques.6
His work came at the time that US President Dwight Eisenhower, suffered a heart attack.
Following the advice of his physician, Eisenhower publicly cut back his fat intake. Nutrition was in the spotlight and Keys was able to further his hypothesis.
This led to radical changes in global food policy and public practice.
In 1977, the USDA Dietary Goals for Americans recommended a decrease in dietary fat intake, and a diet based on grains and cereals.7
At the time, there was still no clinical evidence supporting Keys’ “diet-heart” hypothesis. Subsequent large trials, including the Framingham Study and Women’s Health Initiative Randomized Controlled Dietary Modification Trial, failed to illustrate decreasing dietary fat lowered the risk of heart disease.8,9
Obesity rose following the adoption of the USDA guidelines. Some investigators hypothesized that increased dietary carbohydrates were responsible for the developing health crisis. John Yudkin, a British physiologist and nutritionist, described this phenomenon in his book “Pure, White and Deadly”10–the widespread fear of dietary fats caused scientists and nutritionists to overlook the role of sugar and starch.
Resurgence of ‘Low-Carbohydrate’ Diets
‘Low-fat’ dieting was widespread in the late 1900s. During this time, Dr. Robert Atkins became an infamous spokesperson for the keto diet. Dr. Atkins brought his version of the ketogenic diet to the masses in his 1972 book “Dr. Atkins’ Diet Revolution.” In his 40 years of practice, Dr. Atkins treated an estimated 60,000 patients for obesity and related conditions. At that time, there were no clinical studies to validate the benefits of the diet. Many patients reported side effects while starting the diet, including fatigue, weakness, dizziness, headache, and nausea. This uncomfortable induction phase was labeled the ‘Atkins Flu.’
After Atkins’ death in 2003, others started to promote the ketogenic diet for health. The Atkins Foundation recently funded a group of scientists to study the effects of the Atkins diet formally. This group of scientists includes Jeff Volek, Stephen Phinney, and Dr. Eric Westman. They discovered that the Atkins diet outperformed a diet based on the 1977 USDA guidelines with respect to measured coronary risk factors, including decreased low-density lipoprotein-cholesterol and total blood saturated FFA alongside increased high-density lipoprotein cholesterol.11 This outcome may be due to the decrease in carbohydrate and concomitant changes in the hormonal milieu, or due to effects of ketone bodies on substrate metabolism.
The pendulum of public perception begun to swing in favor of diets higher in fat, thanks to the emergence of influential writers and speakers such as Gary Taubes, Robert Lustig, and Nina Teicholtz, and clinicians and scientists such as Professor Tim Noakes, Dr. Jason Fung, and Professor Thomas Seyfried. The work of these individuals exposed flaws in the ‘diet-heart hypothesis.’
These influencers helped expose corruption in the political decisions that resulted in the last decades of vilification of dietary fat. Evidence illustrating the role of high dietary carbohydrate intake in the development of obesity and diabetes has started to grow. Much of the recent research suggests that low-fat diets may be harmful to health. This culminated with a recent meta-analysis of data from 18 countries, which linked increases in carbohydrate intake with increases in mortality.12
The fear of fat has continued to reverse. Over the last few years, the ketogenic diet has grown in popularity. Popular culture is starting to recognize and adopt the keto diet, and online searches have grown. More and more doctors now encourage and prescribe the ketogenic diet to treat metabolic disorders and obesity. Large online communities bring thousands of people together to discuss research, share keto diet before and after photos, and encourage each other.
Keto Diet for Weight Loss
The ketogenic diet can be used to help with weight loss and also to treat some diseases (discussed in detail elsewhere). Recently, the number of positive keto diet reviews has increased. The rising popularity of the diet has led to a demand for further randomized control trials to study its long-term efficacy. A key reason why the ketogenic diet helps weight loss is that it decreases hunger. This makes it easier to maintain a calorie deficit. It is important to stress that the overconsumption of calories will prevent weight loss, regardless of the macronutrient composition.
Macronutrient Composition of a Keto Diet
Macronutrients are food groups that humans consume in large quantities. They provide the bulk of the energy to the body. The primary macronutrients are carbohydrates, fats, and proteins. The macronutrient composition of a diet can be described using the mass of each macronutrient, the ratio of macronutrients in the diet, or the percentage of each macronutrient in the diet. The variety of descriptions can make things a little confusing!
For example:
- A ketogenic diet contains about 5% of energy as carbohydrates.
- A ketogenic diet has a ratio of 2-4g of fat to every 1g of carbohydrates plus proteins.
- A classical ketogenic diet contains 20-30g of carbohydrate per day
When starting off on the ketogenic diet, these are good target macronutrient ratios:

Examples of food rich in:
- Carbohydrates: bread, pasta, potatoes, cereals, sugary food (sweets).
- Fat: oils (olive oil, coconut oil), butter, fatty cuts of meat, brazil nuts, macadamia nuts, avocado.
- Protein: beef, chicken, pork, fish, milk, cheese, yogurt, eggs.
Carbohydrates
The main function of dietary carbohydrates (‘carbs’) is to be a source of energy. Some say that dietary carbohydrates are not ‘essential’ as they can be made from dietary protein and fat.13

Carbohydrates are biological molecules that contain carbon, hydrogen, and oxygen, usually with a 2:1 ratio of hydrogen:oxygen. Carbohydrates occur as a collection of single units (monosaccharides, e.g. glucose), two molecules joined (disaccharides, e.g. sucrose), and chains of molecules (oligosaccharides and polysaccharides).
When following a ketogenic diet, the carbohydrate intake should be very low.
This contrasts with the modern western diet, where most dietary calories come from carbohydrates. Consuming carbohydrates causes insulin release, which inhibits ketone production in the liver and thus ketosis. Therefore, monitoring and modulating your carbohydrate intake is an important part of following the ketogenic diet.
Dietary carbohydrates replenish the stores in muscle and liver (glycogen). It also maintains blood glucose concentrations to provide fuel for the whole body, but most importantly for the brain.
Blood glucose is easy to measure using a handheld blood glucose monitor. Normal blood glucose levels fluctuate throughout the day and vary between individuals. Therefore, it is useful to track over the long term and in response to different ‘challenges,’ such as a meal or exercise.
Ranges of Blood Glucose levels for clinical diagnosis are as follows:14
- Fasting: healthy = 4-6 mM / 70-110 mgDl
- Fasting: diabetic = ~ 7 mM / 125 mgDl
- 90 minutes post-meal: healthy = < 8 mM / 140 mgDl
- 90 minutes post-meal: diabetics = > 11 mM/ 200 mgDl
When you’re following the ketogenic diet, key concepts are the total amount of carbohydrates, the ‘net’ amount of carbohydrates (accounting for the accompanying fiber), and the speed with which carbohydrates raise blood glucose (glycemic index).
With a standard ketogenic diet, it’s recommended to keep the total amount of carbohydrates limited to less than 5% of energy intake.15 See the table above for a calculation of the advised carbohydrate intake grams for a 2000 kCal per day 4:1 ketogenic diet.
Dietary fiber is carbohydrate-based material from plants that is not entirely broken down by the small intestine. Instead, it passes to the large intestine, and either undergoes fermentation (which supports the growth of beneficial bacteria),16 or excretion.
Fiber is a significant part of a well-formulated ketogenic diet. It helps to maintain gut health, and also increases food bulk and helps with the feeling of ‘fullness.’ Green and cruciferous vegetables are rich in fiber and are helpful to include in a ketogenic diet.
Depending on how ‘complex’ the source of fiber is, it has different assumed caloric values. One approach is to treat fiber as having the same amount of calories per gram as carbohydrates: 4 kCal/gram. However, as a proportion of fiber is not digested, other approaches use a lower value of 2 kCal/g. Digestion-resistant fiber does not contribute to calorie intake, as it is not broken down.
Net carbs refer to the mass of total carbohydrates, minus the total fiber, which could be a better metric to judge carbohydrate intake because:
- Fiber is mostly digestion-resistant and so should not increase blood glucose.16
- Studies have shown an increase in fiber does not affect blood ketone levels.17
The ‘glycemic index’ is a scale that ranges between 1 and 100, and it indicates how quickly food raises blood glucose after consumption. Pure glucose is the reference and is set at 100 (i.e. raises blood glucose quickly). Other foods have a comparatively lower value as they raise blood glucose more slowly. Example values for the glycemic index of food are white potato: ~80, white bread: ~75, apple: ~35, peanuts: ~15.
‘Glycemic load’ accounts for both the speed of carbohydrate release and the TOTAL amount of carbohydrates in food.
Glycemic load = (total carbohydrates (g) x glycemic index) / 1000.
Food can have a relatively high glycemic index (i.e. carrot = 47) but because the total carbohydrate amount is low (carrot = 5g per serving), the glycemic load of one serving is very low.
Proteins
Proteins are large molecules composed of chains of amino acids. The functions of dietary protein are:
- Building structural and functional components of cells
- Conversion to glucose via gluconeogenesis
- Top up intermediates in other metabolic pathways, such as the Krebs Cycle

While it is possible for a protein to be used as a fuel, this isn’t its primary function.
When following a ketogenic diet, there must be a balance of sufficient protein to maintain muscle mass. If dietary protein exceeds 20-25% of calories, gluconeogenesis from protein can stop the ketone production. Initially, target a protein intake of 0.8-1.2g per kilogram of body weight. This target balances the need for protein against the chance of excess gluconeogenesis.18
Some individuals (such as strength or endurance athletes) may have higher protein requirements. They might require a modified ketogenic macronutrient ratio of 2:1 fat:non-fat (where 65% of energy is fat, 30% is protein, and 5% carbohydrate) and can still be effective for therapeutic ketosis.
Fats
Fat gets a bad rap. In nutrition, fat is the dietary macronutrient made up of triglyceride molecules. The main functions of fats in the diet are to provide increased energy levels and makeup key functional and structural parts of the human system.

But we often misuse the word “fat.” There’s a difference between fat in cells and different types of fat molecules:
Adipose tissue: the tissue that stores energy as fats/lipid droplets inside adipocytes (fat cells). This is body fat
- Adipocytes: individual cells that store fats/lipids
- Lipids: the most general term for insoluble and polar biological fat molecules. The lipid class of molecules includes mono-, di- and triglycerols, cholesterols, and phospholipids
- Triglycerides: a lipid molecule made up of glycerol (that acts as a backbone) joined to three fatty acid molecules
- Fatty acids: a molecule composed of a chain of carbon atoms bonded to one another with a carboxylic acid at one end
To be specific, our diet includes many sources of lipids.
Lipids are digested and travel in the blood as triglycerides and fatty acids before being used as a fuel, or stored by adipocytes in adipose tissue. Dietary lipids undergo many tightly regulated metabolic steps before storage in adipose tissue. Dietary fat does not equal stored body fat.
Triglycerides are the most important source of energy in a ketogenic diet. They account for > 70% of dietary calories. For those following a ketogenic diet, it’s helpful to understand how the lipid source in the diet is processed in the body.
Fatty acids can be saturated (no double bonds between carbons), or unsaturated (one or more double bonds between carbons).
Saturated fats are relatively stable and tend to be solid at room temperature (i.e. lard, butter, coconut oil). Historical guidelines recommended limiting the intake of dietary saturated fats because fat consumption was thought to be associated with heart disease and high blood pressure. However, emerging research has shown saturated fat can have beneficial effects on blood biomarkers (i.e. increase ‘healthy’ HDL levels).12
Unsaturated fatty acids can be further divided into monounsaturated fats (only one double bond between carbons) and polyunsaturated fats (multiple double bonds between carbons). The number of double bonds is important as it determines how the fatty acid behaves both inside and outside of the body.
They tend to be liquid at room temperature (i.e. vegetable-based fats such as olive oil). Unsaturated fats are thought of as healthier than saturated fats (also known as “healthy fats”). Increased consumption of mono- and polyunsaturated fats have been linked to improved blood biomarkers (i.e. lower blood triglycerides).19 Eating enough unsaturated fats is important when following a ketogenic diet.
Increased fat consumption is not associated with cardiovascular disease.20
Eating a moderate amount of saturated fat is unlikely to be as harmful as previously believed, and saturated fat consumption as part of a ketogenic diet is unlikely to increase the risk of cardiovascular disease.
Trans-fats are produced artificially when hydrogen is added to unsaturated fatty acids in order to solidify it and make it last longer. Because of associations with poor health outcomes, these artificial fats had their generally regarded as safe (GRAS) status removed in 2015 by the FDA. 21 Avoid high levels of trans-fat consumption by eating a diet based around whole foods.
Essential fatty acids are important to include in the diet because the body cannot naturally produce them. This group includes poly-unsaturated omega 3, omega 6, and omega 9 fatty acids.
It’s believed the anti-inflammatory effects of essential fatty acids may have broad benefits for health and performance. Oily fish, such as sardines and mackerel, and seeds (i.e. flax) are good dietary sources of essential fatty acids.
The number of carbons in the fatty acid chain also has an important effect on its metabolism. The carbon chain of fatty acids can be up to 28 carbons atoms long. If there are > 13 carbons in the fatty acid, it is called a long-chain fatty acid, between 8-12 is a medium-chain fatty acid, and under 5 carbons is a short-chain fatty acid.
The body metabolizes fats differently according to chain length. Long-chain fatty acids are absorbed and go from the gut into the lymphatic drainage system and from there are released directly into the blood.
By comparison, medium- and short-chain fatty acids do not go into the lymphatic system. They travel in the blood from the gut directly to the liver.22 If a large amount of these short- and medium-chain fats are delivered to the liver at once, this can trigger the liver to convert them into ketones, even without dietary carbohydrate restriction.
Medium-chain fatty acids are highly ketogenic. They can be found in natural sources such as coconut oil or in an artificially purified form. However, for many people, consuming a high amount of medium-chain fatty acids can cause an upset stomach. This limits their use to raise ketones artificially.
When integrating these concepts into a ketogenic diet: target the majority of dietary calories as fat.
Aim to include a variety of fats from different animal and plant sources (i.e. red meat, poultry, fish, dairy, olive oil, coconut oil, nuts, and avocados).
Conversely, micronutrients must be obtained in the diet in small quantities, but are essential to health. Vitamins and minerals are examples of micronutrients.
Micronutrients in a Ketogenic Diet

When following a ketogenic diet, it is important to be mindful of micronutrient intake because:
- Reducing carbohydrate intake can lower consumption of micronutrient-rich foods (i.e. fruits and vegetables)
- In the initial 28 days of following a ketogenic diet, the balance of some micronutrients (such as sodium, potassium, magnesium, and calcium) can become disturbed due to an increase in their excretion.23 The body resolves this issue naturally after adapting to the diet
Sodium is the principal cation in extracellular fluid. Its functions are related to blood volume maintenance, water balance, and cell membrane potential. Sodium is also essential for acid-base balance and nerve conduction.
The level of sodium can fall at the start of a ketogenic diet. Adding extra sodium to meals (like adding salt or consuming bouillon/ bone broth) can reduce the chances of feeling the common side effects associated with low sodium (like cramps).
Potassium is the principal cation in the intracellular fluid. Its primary functions are related to maintaining cell membrane potential and electrical activity in cells such as neurons and cardiomyocytes.
As with sodium, levels of potassium fall at the initiation of a ketogenic diet due to increased excretion. When starting a ketogenic diet, include sources of potassium like nuts, dark green vegetables, and avocados.
Magnesium is an essential element in biological systems, especially for nerve, muscle, and immune function. Levels of magnesium also fall at the initiation of a ketogenic diet due to increased excretion. When starting a ketogenic diet, include sources of magnesium like oily fish, dark green vegetables, and seeds.
Calcium has a role in muscle contraction and is important for cardiovascular and bone health. Calcium deficiency is less common during a ketogenic diet, as staples of the diet such as fish, cheese, and leafy greens are rich sources of the mineral.
Now that an understanding of the biology of the ketogenic diet has been reached, we’ve arrived at the fun part: how to start the keto diet.
Keto Diet for Weight Loss
There’s a growing consensus that the keto diet can help with weight loss.
The rising popularity of the diet has led to a demand for further randomized control trials to study its long-term efficacy. The ketogenic diet helps weight loss because it decreases hunger. This makes it easier to maintain a calorie deficit. It is important to stress that the overconsumption of calories will prevent weight loss, regardless of the macronutrient composition.
How to Start a Ketogenic Diet
Don’t try to start the diet gradually. If carbohydrate intake is moderately-low, blood sugar levels may not be enough to fuel the brain, and the presence of carbohydrate in the diet might still be enough to stop the body from making ketones.
The main objectives when starting the ketogenic diet are to:
- Restrict carbohydrates to 20 digestible grams per day or less – a strict low-carb diet
- Consume plenty of fiber
- Restrict protein to moderate levels. If possible, stay at or below 0.45 grams of protein per day, per lb of body weight (1g/kg). So about 70 grams of protein per day if you weigh ~155 lbs (~70kg). If your goal is to lose weight, aim for 1 gram of protein per kg of your target weight
- Consume fat until you are satiated
Tips for Starting the Ketogenic Diet
- Make a keto diet menu. It’s a good idea to keto meal plan before starting the diet. Make a shopping trip to stock up on a range of foods that are low in carbohydrates and high in fat
- Use an app to track macronutrient intake. Apps such as MyFitnessPal are great to get an idea of the macronutrients in common foods. There is also a range of special online keto diet calculators
- Search for a few keto recipes to adapt cooking methods. Due to the high-fat consumption required to get into ketosis, it may be beneficial to change daily staples or cooking methods. Keep an eye out for coconut oil, heavy cream, and lots of cheese
- Make an approved list of keto foods and eliminate carbohydrate-rich foods. It will be easier to follow the diet by throwing out any foods to avoid. It’s recommended to check the labels for hidden added sugars
- Consider starting the ketogenic diet within a short period (16-36 hours) of fasting (consuming zero calories). Fasting depletes carbohydrate stores and can accelerate ketone production. Click here to read more about fasting protocols
- Gentle cardio exercise (~30 minutes) or some short high-intensity intervals (10-second sprints) can deplete carbohydrate stores and speed up ketone production

Cyclical Ketogenic Dieting and ‘Cheating’
At the moment, there is not a clear answer as to whether the benefits of the ketogenic diet can be achieved by cycling on and off the diet. It’s best to stick to the diet for 1-2 months minimum to see benefits. It can take several days to get into ketosis1 and 3-6 weeks to become “fat adapted.”18
Some research indicates ~40 days on the ketogenic diet interspersed with periods of healthy eating with more carbohydrates (Mediterranean diet) could maintain weight loss.24
“Cheating,” and consuming high-carbohydrate food, quickly stops ketone production by the liver. It can then take a considerable amount of time for the body to get back into ketosis. Time taken to get back into ketosis will depend on many factors. These include the amount of carbohydrates consumed, how adapted the body is to produce ketones, activity level, etc.
However, cyclical ketogenic diets are a promising area of scientific investigation. Recently, scientists studied the effect of long-term cycling of the ketogenic diet (one week on, one week off the diet) compared to a normal diet in mice. Cyclical keto dieting reduced mid-life mortality and increased healthspan.25
Optimal Range of Ketosis
As with all processes in metabolism, the state of ketosis is a spectrum. Past a threshold (which varies from person to person), even a small increase in dietary carbohydrate intake can trigger enough insulin release to take the body out of ketosis.
Guidelines for target levels for blood ketones are:
- No ketosis: under 0.5 mM BHB in blood
- Low ketosis: 0.5 – 1.5 mM BHB in blood
- Moderate ketosis: 1.5 – 3 mM BHB in blood
- High ketosis: over 3 mM BHB in blood
Pathological ketosis: over 15 mM BHB in blood
The level of ketosis required for different physiological benefits is unknown. For endurance sports, a higher level of ketosis (~4 mM) appears to be superior to lower levels.26,27 This is possible because ketones fuel athletes.
However, some other benefits of ketosis, such as reduced appetite may be seen at much lower levels (0.5 mM).28
The best way to know if you are in ketosis is to measure the levels of ketones (BHB) in your blood. You can also estimate blood levels by measuring ketones in your breath or urine.
Physiological Ketosis
The typical methods used to generate physiological levels of ketosis are fasting, the ketogenic diet, and consuming exogenous ketones like HVMN Ketone.
After an overnight fast, a low amount of ketones (0.1-0.2 mM) can often be detected in the blood. As the time spent fasting increases, blood ketone levels slowly rise until a plateau at 8-10 mM of BHB has been reached after many days. Scientist Hans Krebs described this plateau as “physiological ketosis.”29
Fasting long-term is unsustainable, so following a strict ketogenic diet can be used to maintain a low level of continuous ketosis. Research suggests blood BHB levels between 0.4-1mM can be achieved while following a ketogenic diet.18 Anecdotal evidence suggests it’s sometimes possible to reach higher levels.
Using exogenous ketones can raise blood ketones to a physiological level without the ketogenic diet or fasting. The level of ketosis reached depends on the exogenous ketone supplement used. Reported levels range from 0.6 mM with a ketone salt or a medium-chain triglyceride supplement26,30 and up to 6 mM with HVMN Ketone.27
Pathological Ketosis
Sometimes, the body starts producing ketones as a result of a disease (pathology). This can lead to dangerous levels of ketones in the body, though these high levels are very uncommon in healthy people following the ketogenic diet.
Alcoholic ketoacidosis (AKA) is a result of chronic alcohol consumption usually accompanied by malnutrition. AKA is characterized by increased ketone production (levels > 15 mM) via liver alcohol metabolism, in conjunction with a mild elevation in blood glucose levels. Symptoms include nausea and vomiting, fatigue, altered breathing, and abdominal pain.31
Diabetic ketoacidosis (DKA) occurs most frequently in patients with type 1 diabetes. DKA is the simultaneous occurrence of high blood ketones (> 20 mM), high blood glucose, and acidification of the blood.31 It develops when insulin is absent, or insulin signaling is no longer functional.
This means the physiological state of starvation is triggered, even in the presence of high blood glucose. As during starvation, lipolysis (fat release) increases. This causes the liver to produce a high amount of ketones and blood pH to fall (as ketones are an organic acid).
As glucose levels are very high, the excess is excreted in the urine. This draws water and electrolytes out of the body, causing dangerous dehydration. Symptoms of DKA include nausea, vomiting, altered breathing, abdominal pain, and unconsciousness. The rapid onset and alarming nature of DKA is a reason why ketosis has a bad stigma in the medical community.
Who Should Avoid a Ketogenic Diet?
Following a ketogenic diet may not be suggested for people with the following medical considerations:
- Pregnancy
- Kidney failure
- Impaired liver function
- Impaired fat digestion (gallbladder disease, gastric bypass, pancreatitis)
Genetic defects in metabolism (CPTI/II deficiency, beta-oxidation defects, fatty acyl dehydrogenase deficiency)
Potential Side Effects of the Ketogenic Diet
When starting a ketogenic diet there can be a period of 2-3 days where blood glucose levels are low, but ketone production has not reached a sufficient rate to provide enough fuel for the brain.
This can result in a series of symptoms, known as the keto flu, which include:
- Headache
- Muscle cramps
- Fatigue
- Nausea
- Dizziness
Exogenous ketone supplements, such as HVMN Ketone, and medium-chain triglycerides can be used to reduce symptoms of keto flu. They provide the brain with a source of energy without carbohydrate consumption. These supplements increase the levels of ketones in the blood artificially. Exogenous ketones do not increase the body’s ketone production (called endogenous ketones) and can inhibit32 the release of fatty acids from adipocytes.
It can be initially tricky to adjust food intake to ensure adequate nutrition when following a ketogenic diet. Also, some people find the diet isn’t sustainable due to individual differences in metabolic state or lifestyle. If the diet does not provide the correct balance of macro and micronutrients, some individuals develop other symptoms beyond the keto flu after the adaptation period. These include:
- Constipation
- Bad breath
- Difficulty in maintaining physical performance
- Hair loss
- Gallstones
- Elevated blood triglycerides or cholesterol
To treat these symptoms, ensure the diet provides enough calories and micronutrients. Many people reduce fruit and vegetable consumption on a ketogenic diet (due to carbohydrate content). This means it is easy to become deficient in vitamins and to under-consume fiber.
The ketogenic diet can alter the way that the kidneys excrete electrolytes (such as sodium), so electrolyte supplementation can reduce the side effects of an electrolyte imbalance.
Possible Clinical Applications of the Ketogenic Diet and Ketosis
Some of the earliest reports of the ketogenic diet describe its use in a clinical setting.
In the early 20th century, ketogenic diets helped treat drug-resistant epilepsy. Doctors also prescribed ketogenic diets to treat type 1 diabetes before the invention of insulin.
As analytical techniques progressed, scientists learned that ketones themselves might be a crucial part of the success of the ketogenic diet to treat disease. From this finding stemmed a field of research to examine the potential benefits of ketosis in a range of disease states:
- Weight loss
- Diabetes and metabolic syndrome
- Neurological disease: epilepsy, Alzheimer’s disease, Parkinson’s disease, migraine, concussive disease, and traumatic brain injury
- Cancer
- Inflammatory diseases
While the ketogenic diet is not yet a first-line treatment recommended by doctors for any of these diseases, it’s a relatively easy and tolerable step that patients with these conditions can take to improve their health. Emerging research suggests there may be beneficial effects of ketosis for some people, and further studies are required to confirm how best to use the diet in these clinical settings.
Scientific Citations